
Altis® Single Incision Sling
Confidence & Control
For you and your patients

Underreported.
Underdiagnosed.
Undertreated.
An estimated 53.6 million women in the U.S. suffer from stress urinary incontinence or mixed urinary incontinence.
Some women feel too embarrassed or that their incontinence isn’t severe enough to see a physician, while others aren’t aware of their treatment options, meaning too many women aren’t getting the life-changing help they need. Less than 1% go onto have surgery, despite low quality of life, including depression and anxiety.3
More than an inconvenience
Urinary Incontinence can have profound impacts on a woman’s life.
2/3
of women with SUI adopt precautionary routines to reduce the chance of leaking in public
32.3%
of working-aged women with SUI avoid sexual activity
25-50%
of women with SUI experience anxiety or depression
Surgery
for SUI decreased anxiety by 1/2 and depression by 2/3
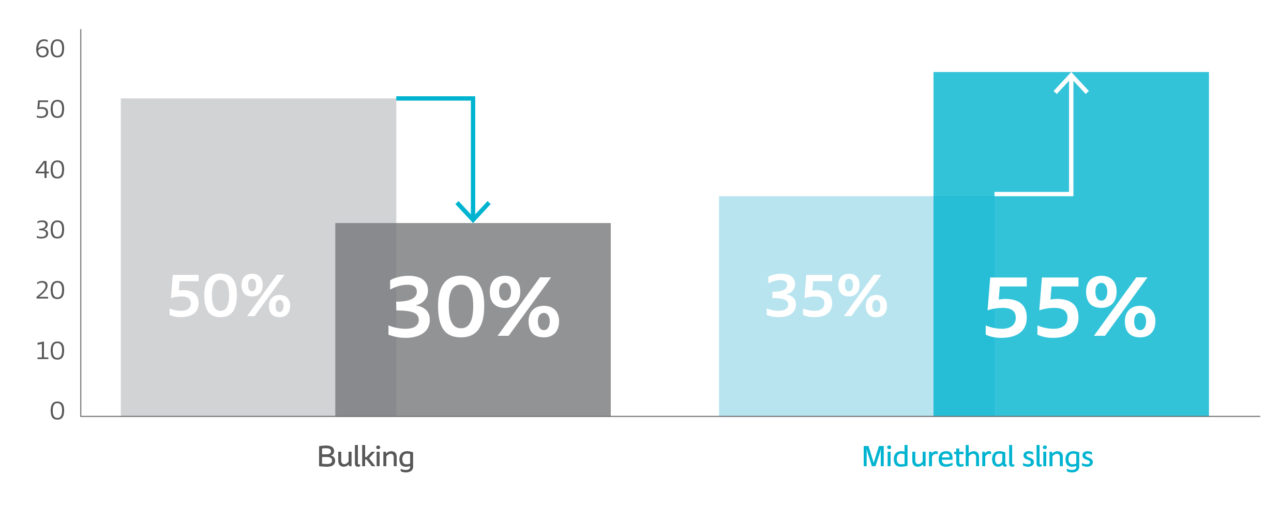
Certain concerns may cause women to choose a less invasive option
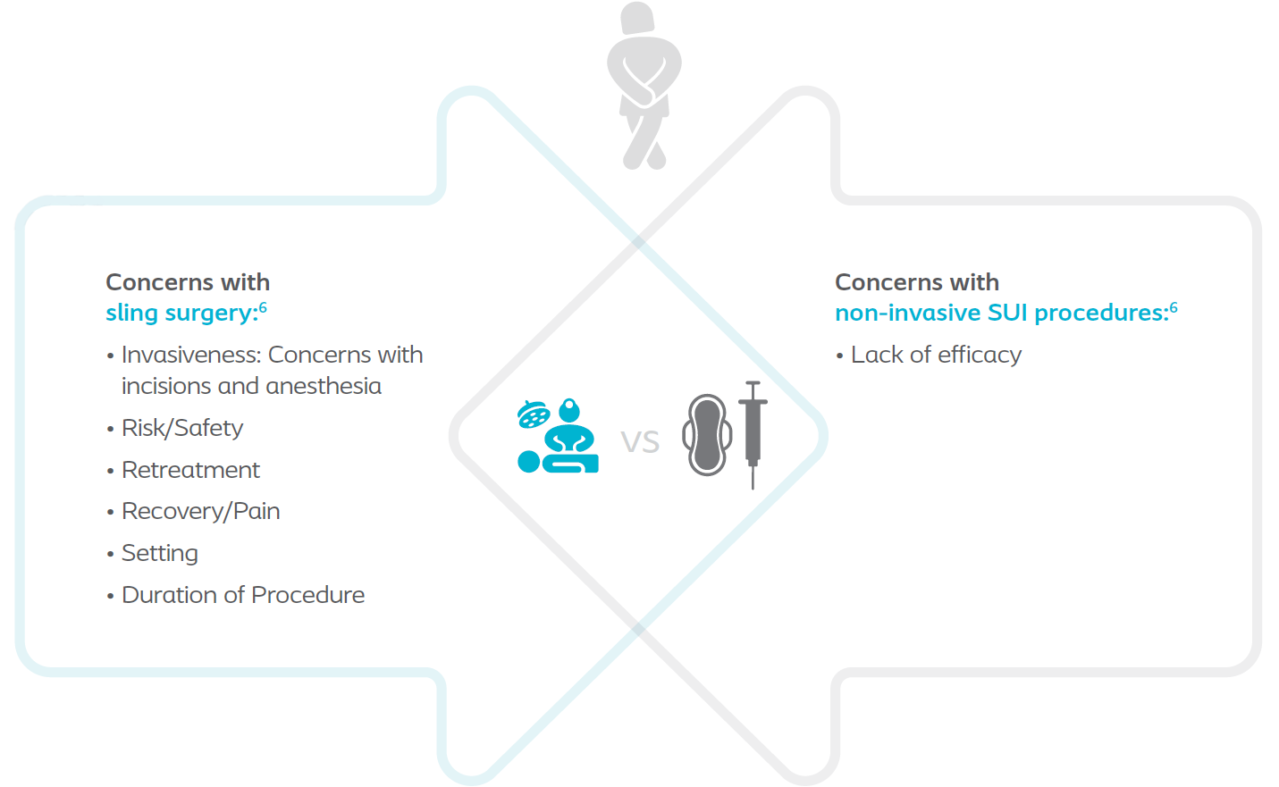
When initially being offered the option of bulking versus a midurethral sling (MUS), 50% of women preferred bulking vs. 35% to MUS.
However, when they heard the difference in efficacy, 30% preferred bulking and 55% preferred MUS.6
The real-life advantages of single incision slings
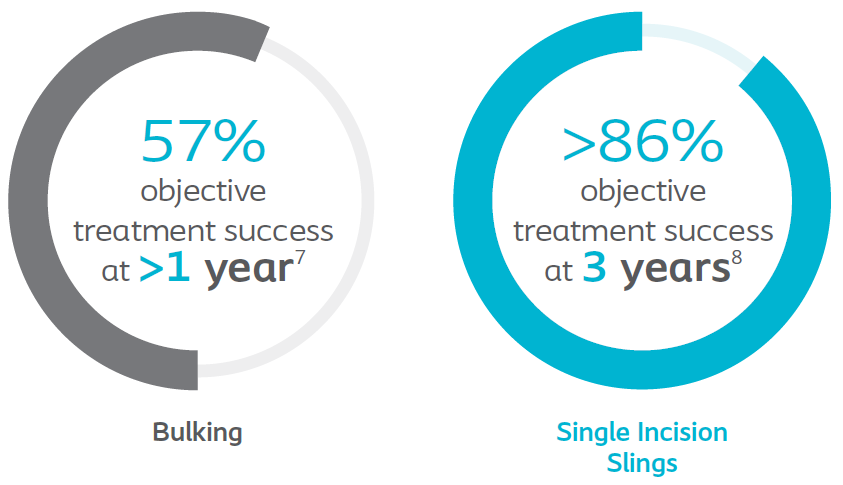
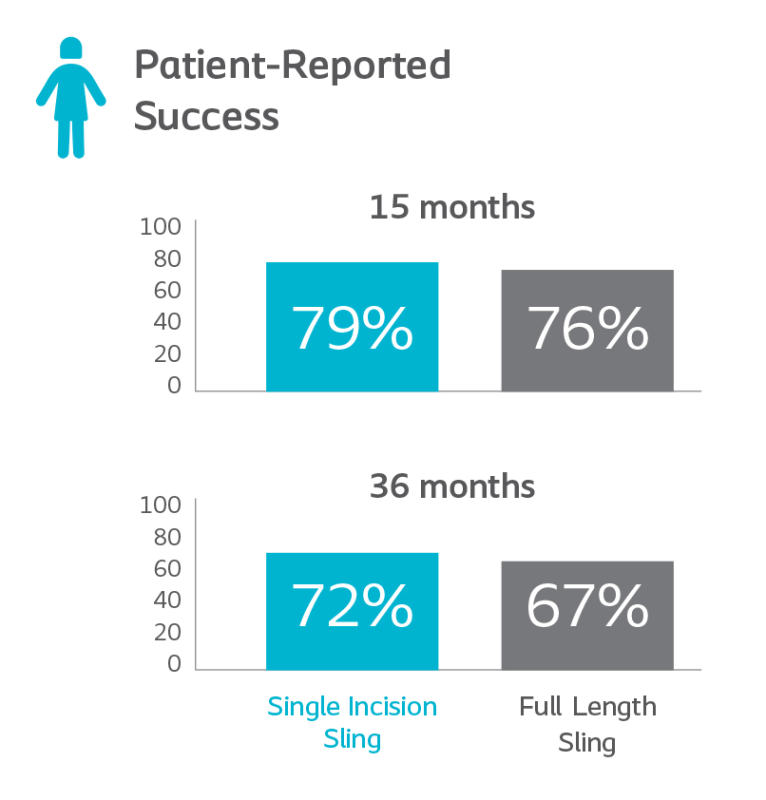
Similar results, better patient experience
According to the NEJM, single incision slings were found to have similar rates of objective success and patient-reported success to full length slings.

Compared to full length slings:
Better Patient Experience
- Women with single incision slings had less post-op pain up to 14 days.
- Compared to full length slings, women receiving single incision slings were able to return to normal activities on average 5 days sooner.
- Minimally Invasive
Single incision slings involve fewer incisions and less tissue trauma than traditional full length slings and can be implanted under local anesthesia in an outpatient setting. - Sexual Function
Studies have shown there may be an improvement in sexual function for both single incision slings and full length slings.10
Less Procedure & Hospital Time
- Single incision sling procedure patients are associated with5% less procedure time and 26% less post-op recovery time.
- Better Post-Op Voiding Results
Higher rates of postoperative voiding dysfunction are associated with retropubic slings. - Single incision slings reported less bladder and urethral injury during surgery, with comparable results to full length slings in number of post-operative serious adverse events.
Change perceptions. Change lives. Altis® is your alternative.
The control you need.
The confidence you want.
The choice your patients deserve.
The Altis® Single Incision Sling System is a unique, minimally invasive solution purposefully designed to provide predictable placement and adjustable control. This makes the procedure straightforward, accurate and repeatable.

LESS INVASIVE
One incision. Less tissue trauma. Speed up procedure time and deliver a better patient experience.
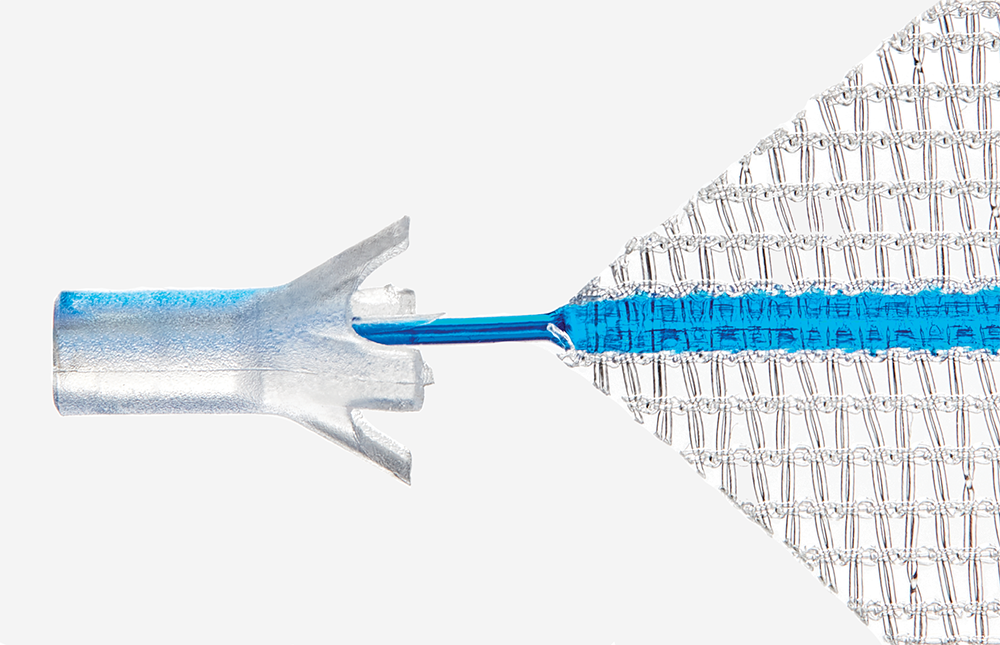
STABLE SUPPORT
This flexible patented mesh is the thinnest and lightest SUI mesh available, allowing support of the urethra.
The most
rigorously studied
single incision sling in the U.S
At 24 months, the Altis Single Incision Sling is comparable to full length retropubic and transobturator slings and is the only sling to have a premarket IDE and 522 study
Altis® Single Incision Sling Brief Statement
Indications
The Altis® Single Incision Sling System is indicated for the treatment of female stress urinary incontinence (SUI) resulting from urethral hypermobility and/or intrinsic sphincter deficiency (ISD).
Contraindications
It is the responsibility of the physician to advise the prospective patients or their representatives, prior to surgery, of the contraindications associated with the use of this product. The Altis Single Incision Sling System is contraindicated for use in patients with the following conditions:
- Pregnancy or desire for future pregnancy
- Potential for further growth (e.g., adolescents)
- Known active urinary tract infection and/or infection in operative field
- Taking anti-coagulant therapy
- Abnormal urethra (e.g., fistula, diverticulum)
- Intraoperative urethral injury
- Any condition, including known or suspected pelvic pathology, which could compromise implant or implant placement
- Sensitivity/allergy to polypropylene
Warnings and Precautions
It is the responsibility of the physician to advise the prospective patients or their representatives, prior to surgery, of the warnings and precautions associated with the use of this product and the associated surgical risks.
Warnings
The Altis® Single Incision Sling System should only be used by physicians familiar with the surgical procedures and techniques involving transvaginal placement of non-absorbable, synthetic mesh slings and who have adequate education and experience in the treatment of female SUI.
A thorough assessment of each patient should be made to determine the suitability of a synthetic mesh sling procedure.
The patient should be counseled that alternative incontinence treatments may be appropriate, and the reason for choosing a mesh sling procedure should be explained.
Obtain patient consent prior to surgery and ensure that the patient has an understanding of the postoperative risks and potential complications of transvaginal mesh sling surgery.
Patient counseling should include a discussion that the sling to be implanted is a permanent implant and that some complications associated with the implanted mesh sling may require additional surgery; repeat surgery may not resolve these complications. Serious adverse tissue responses or infection may require removal of mesh, and complete removal of the sling may not always be possible. Individuals may have varying degrees of collagen laydown that may result in scarring.
As with all surgical procedures, patients with certain underlying conditions may be more susceptible to postoperative bleeding, impaired blood supply, compromised/delayed healing, or other complications and adverse events.
The risks and benefits of using Altis should be considered in patients.
Any future pregnancy could negate the benefits of this surgical procedure. Patients should report any bleeding, pain, abnormal vaginal discharge or sign of infection that occur at any time.
The procedure to insert the Altis sling requires good knowledge of pelvic anatomy and the correct use of the introducer needles in order to avoid damage to adjacent anatomical structures.
Cystoscopy should be performed to confirm bladder and urethral integrity.
Avoid placing excessive tension on the Altis sling during placement and adjustment to maintain sling integrity and to avoid compression of the urethra when tensioning.
Potential Complications
Potential complications include mesh extrusion, pelvic/urogenital pain, groin pain, hip pain (may be related to patient positioning), urinary retention, bleeding, de novo urgency, delayed wound healing, dyspareunia, hip/groin pain, inflammation, nausea, overactive bladder, pain, pelvic hematoma, reaction to antibiotic, slight discomfort upon return to work, urinary tract infection, urine stream decreased, and voiding dysfunction.
Adverse events are known to occur with transvaginal synthetic sling procedures and implants. Adverse events following mesh implantation may be de novo, persistent, worsening, transient, or permanent.
Additional potential complications include, but are not limited to, abscess (acute or delayed), adhesion/scar formation, allergy, hypersensitivity or other immune reaction, bleeding, hemorrhage or hematoma, dehiscence, delayed wound healing, extrusion, erosion or exposure of mesh sling into the vagina or other structures or organs, fistula formation, infection, inflammation (acute or chronic), local irritation, necrosis, de novo and/or worsening dyspareunia, neuromuscular symptoms (acute or chronic), partner pain and/or discomfort during intercourse, perforation or injury of soft tissue (e.g., muscles, nerves, vessels), structures, or organs (e.g., bone, bladder, urethra, ureters, vagina), seroma, sling migration, suture erosion, bladder storage dysfunction (e.g., increased daytime frequency, urgency, nocturia, overactive bladder, urinary incontinence), ureteral obstruction, urinary tract infection, voiding symptoms (e.g., dysuria, urinary retention, incomplete emptying, straining, positional voiding, weak stream), granulation tissue formation, palpable mesh (patient and/or partner), sexual dysfunction, vaginal discharge (abnormal) and vaginal scarring or tightening.
The occurrence of these events may require one or more revision surgeries, including removal of the sling.
Complete removal of the sling may not always be possible, and additional surgeries may not always fully correct the complications.
There may be unresolved pain with or without mesh sling explanation.